Analysts believe Amazon, JPMorgan Chase, and Berkshire Hathaway's proposed partnership could start with a relatively modest internal health insurance offering and build upon that.
Amazon's anticipated venture into healthcare has the potential to disrupt traditional markets, especially pharmacy, pharmacy benefits, and supply chain, Standard & Poor's analysts say.
However, the Byzantine nature of the nation's $3.3 trillion healthcare sector will also determine the pace of that disruption.
"Given the sheer complexity of healthcare and its importance to our economy, change doesn't really come fast," Shannan Murphy, director of Corporate Healthcare Sector for S&P Global, said in a conference call Thursday.
"That said, we do think that change is coming slowly but surely, and certain elements of healthcare are more or less ripe for near-term disruption," Murphy said.
The vaguely worded announcement late last month that Amazon, JPMorgan Chase, and Berkshire Hathaway would create a nonprofit entity designed to reduce their employees' healthcare costs sent shivers through the pharmacy, pharmacy benefits, and supply sectors, with a loss of about $69 billion in market cap that day.
The market slide underscored investor jitters about sustainable margins given healthcare business models that provide limited pricing transparency, S&P says. However, the trio provided few details for their plans, which S&P analysts believe could start with an internal insurance offering and build upon that.
"All three companies are likely self-insured so they could try to tackle ancillary insurance services such as PBM," said Tulip Lim, director of S&P's corporate healthcare ratings. "This could help Amazon, especially if they wanted to get into the area of prescription drugs."
"But it's probably more likely that they would buy a PBM rather than build one, because operating a PBM requires certain competencies outside of the three's core, such as formulary management," she said.
The sectors most at risk for disruption are distributors of lab and medical supplies, but that comes with caveats.
"Even though Amazon is an e-commerce powerhouse, it might take a while before they take meaningful shares from certain rated players," Lim said. "That's because many of these companies cater to the acute-care market, which will be slower to buy meaningfully from Amazon."
"The distributors are pretty intertwined with the hospitals and are also pretty efficient at delivering products in large quantities and on short notice," she said. "Plus, many of the distributors provide additional services; specialized sales people, customized products, and a breadth of products like medical supplies and drugs."
Lim said Amazon would face hurdles entering the retail prescription drug market, even though they already have the Amazon RX domain name, and they’ve been in talks with generic drug manufacturers.
"In terms of pharmacy, Amazon has already been impacting the retailers in the nonprescription drug area and they could use Whole Foods as part of a pharmacy strategy," she said. "But, we think they would have to partner with a PBM to gain any real volume. Otherwise, they could only reach the cash-pay market, which is relatively small."
That might be a big hurdle because the biggest retailers have their own competing mail order pharmacies.
Lim says the wholesale drug distribution business would seem like a logical inroad for Amazon because it's good at order taking and fulfillment. But that is not the only function of wholesalers. "They also use their scale to buy drugs at a discount. Starting out amazon wouldn't have that scale unless they bought someone," she said. "Even the biggest pharm chains have thought it was best to join forces with a distributor to buy drugs."
Amazon could also shake things up in the healthcare sector by by following through on its promise to provide market transparency.
"That is maybe one of the reasons why investors are spooked because this is a very opaque marketplace," Lim said. "There are a lot of different companies involved and there are third-party payers involved and different middlemen involved. That is part of the reason for the complexity."
The Franklin, Tennessee–based for-profit hospital chain has sold another asset as part of its ongoing efforts to reduce about $1.5 billion in debts. The sale of Byrd Regional Hospital leaves CHS with one hospital in Louisiana.
Community Health Systems Inc. has sold a hospital in Louisiana to privately held Allegiance Health Managementas part of its ongoing efforts to pay down about $1.5 billion in debts, the company said.
Byrd Regional Hospital is a 60-bed hospital in Leesville, Louisiana. The deal includes physician and outpatient services, and is expected to close by June, pending regulatory approval. Financial terms were not disclosed.
Franklin, Tennessee–based CHS said Byrd Regional was one of the planned sales discussed on the company’s third quarter 2017 earnings call. The sale leaves CHS with one hospital in Louisiana, the 159-bed Northern Louisiana Medical Center in Ruston.
CHS has struggled financially since the $7.6 billion acquisition of Health Management Associates in 2014. At the time, the deal made CHS the largest for-profit hospital chain in the nation. Since then, CHS has sold more than 30 hospitals and plans are underway to sell more.
"Based on the facts and circumstances at the time, I certainly would do the deal. Based on a retro view of it, I wouldn't do the deal," Smith said.
Although some investors have called for Smith to resign, Shanda Group, a Chinese private equity firm with a 24% stake in CHS, expressed support for Smith.
"We have consistently maintained a good relationship with (CHS) and are supportive of the company and its management team as they continue to execute on the company's strategic objectives," Shanda President Robert Chiu said in amedia release.
CHS shares have rebounded slightly in 2018, and were trading at around $5.50 this week on the New York Stock Exchange, from a low of about $3.85 a share in early January.
With the acquisition of Byrd Regional, Shreveport, Louisiana–based Allegiance Health will operate six hospitals in Louisiana. The company operates 12 acute-care, long-term care, or behavioral health facilities in Louisiana, Texas, Arkansas, and Mississippi.
Private insurance spending for hospital care is decelerating, owing to aging Baby Boomers transitioning to Medicare, the impending repeal of the individual mandate, and the growth of high-deductible plans that constrain utilization.
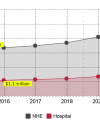
Hospital spending will grow about 5.5% each year, from $1.3 trillion in 2018 to $1.8 trillion in 2026, driven largely by an aging demographic and price increases, according to Centers for Medicare & Medicaid Services projections.
Hospital spending grew by 4.6% and 4.7% in 2016 and 2017, respectively, CMS said.
"While growth is expected to be the same or somewhat faster for most major payers for hospital care, including Medicare/Medicaid, growth for private health insurance spending for hospital care is expected to slow by 0.9 percentage points in 2017," CMS economist Andrea Sisko said Tuesday.
"That is due, in part, to the effect of high-deductible health plans on utilization that was more than offset by the Affordable Care Act coverage expansion in 2014 through 2016," Sisko said.
The 0.9 percentage point deceleration is also projected for private health insurance spending for physician and clinical services, Sisko said.
“Otherwise, growth in projected prices and demographics are some of the factors driving spending by payers for the remainder of the projection period,” she said.
In 2017, 28% of workers were enrolled in high-deductible plans, compared with 5% in 2007, and CMS said there is increasing evidence that enrollment in high-deductible plans constrains the use of healthcare goods and services, particularly after the initial enrollment shift.
"The share of private health insurance enrollees in high-deductible plans is anticipated to stabilize over the projection period," CMS said. "Consequently, by the latter half of the period, both out-of-pocket and private health insurance spending for personal healthcare are projected to be driven by the same underlying factors (most importantly, disposable personal income that affects the use of healthcare goods and services)."
Spending for hospital care is projected to increase from $970 billion in 2018 to $1.8 trillion in 2026, while spending for physician and clinical services is expected to climb from $734 billion to $1.1 trillion over the same eight years.
CMS economist Gigi Cuckler said that many of the drivers affecting hospital spending are also affecting physician and clinical services.
"In 2017 you had the effect of the coverage expansion dampening and you start to see the effects of the proliferation of high-deductible plans, particularly on private health insurance spending," she said.
"So, you have a slowdown in projected private health insurance spending for 2017 which, in turn, results in a slowdown in overall physician and clinical services projected growth to 5% in 2017, from 5.4% in 2016," she said.
"By 2018, however, we are projecting that prices for physician and clinical services will increase largely due to increases in overall economy-wide inflation, but also due to increases in input prices, in particular healthcare wages," she said.
Even with the increase in prices projected for 2018, CMS projects a modest increase in growth for physician and clinical services, from 5% in 2017 to 5.1% in 2018.
"In 2019-20 private health insurance growth is dampened by the repeal of the individual mandate, while out-of-pocket spending is projected to increase. That is something we see similarly flow through to a lot of the sector," Cuckler said.
Closer to 2026, Cuckler said, "the trends in private health insurance and out-of-pocket spending are mostly driven by the same underlying factors that typically contribute to growth in spending in this category, mainly the lag effect of disposable personal income growth."
Medicare growth is also projected to accelerate in the second half of the projection, Cuckler said, which is partly related to physician incentive payments under the MACRA legislation and the end of sequestration, which explains an uptick in growth for Medicare physician spending in 2026.
If the current pace holds, CMS actuaries project healthcare spending will reach $5.7 trillion by 2026 and consume nearly 20% of the gross domestic product.
Healthcare spending is projected to eat an even bigger slice of the U.S. economy in the next eight years, according to projections released today by the Centers for Medicare & Medicaid Services.
CMS' Office of the Actuary projects an average annual rate of national health spending growth of 5.5% for 2017–26, representing about $5.7 trillion, and outpacing average projected growth in gross domestic product by 1 percentage point.
The key drivers for spending growth include: growth in disposable personal income; increased prices for medical goods and services; and aging Baby Boomers’ ongoing shift from private health plans to Medicare, CMS said.
As a result, the healthcare share of the economy is projected to climb to 19.7% by 2026—up from 17.9% in 2016, or $3.3 trillion. CMS said the projections rely on the current-law framework and assume no legislative changes over the decade.
"Something that really stands out is how much these projections are really influenced by fundamental demographic and economic shifts," Gigi Cuckler, an economist at CMS and lead author of the study said Tuesday in a media conference call.
"It’s very clear that the aging of the population has a significant influence on Medicare enrollment and shifts out of private health insurance. And it is also very clear that the growth in income, particularly disposable personal income, has a substantial influence, particularly on projected private health insurance and out-of-pocket spending," she said.
Along with the aging demographic, price growth for medical goods and services is also expected to be a significant factor for spending growth, and is projected to increase from historically low rates in 2014–16 of 1.1% per year, and average 2.5% per year for 2017–26.
Spending for hospital care is projected to increase from $970 billion in 2018 to $1.8 trillion in 2026, while spending for physician and clinical services is expected to climb from $734 billion to $1.1 trillion over the same eight years.
Prescription drugs will see the fastest average annual spending growth over the eight years, at 6.3% per year, growing from $360 billion in 2018 to $605 billion in 2026, largely because of increased spending on specialty drugs.
The insured share of the population is expected to decline slightly from 91.1% in 2016 to 89.3% in 2026, due to the repeal of the Affordable Care Act’s individual mandate.
Here is a chronological look at projected trends:
2018
National health spending growth is projected to increase to 5.3%, up from 4.6% in 2017.
Medicaid spending growth is projected to increase 4 percentage points, at a projected rate of 6.9%, due to the growth in health insurance spending as a result of smaller risk-mitigation recovery payments from the previous year.
Private health insurance spending growth is projected to decelerate to 4.8%, down from 5.6% in 2017, due to slower growth in the net cost of insurance in the Marketplace.
Prescription drug spending growth is anticipated to accelerate from 2.9% in 2017 to 6.6% in 2018, based on the expectation that the dollar value of drugs losing patent protection is less than in previous years.
2019–20
National health spending growth is projected to average 5.5%, a slight acceleration from 5.3% in 2018, as a result of faster projected average growth in Medicare spending not fully offset by slower average growth in private healthcare insurance spending.
Compared to 2018, Medicare spending is projected to grow 2 percentage points faster on average at 8%, reflecting accelerated physician incentive payments under MACRA, and projected growth in the use and intensity of Medicare goods and services.
Private health insurance spending is projected to slow on average to 4.1%, from 4.8 percent in 2018, due in part to the repeal of the individual mandate.
The number of uninsured people is projected to increase to 32.7 million by 2020, rising from 30 million projected for 2018.
2021–26
National health expenditure growth is projected to accelerate and average 5.7%, up from 5.5% projected for 2019–20.
Average Medicare and Medicaid spending growth (7.7% and 6.1%, respectively) will continue to outpace that of private health insurance (4.7%) due to the aging of the population, including continued strong enrollment growth.
In 2026, 47% of national health spending is projected to be sponsored by federal, state, and local governments, up from 45% in 2016. This reflects the shifting demographics including the continued transition of Baby Boomers to Medicare.
The projected share of health spending by businesses, households, and other private revenues is expected to fall 2 percentage points, from 55% in 2016 to 53% in 2026.
Filefax, Inc. took medical records to a shredding facility but failed to properly dispose of the documents, which contained protected health information from about 2,150 patients.
A receiver appointed to liquidate the assets of a bankrupt medical records storage company will pay $100,000 to settle potential violations of the Health Insurance Portability and Accountability Act, the Department of Health and Human Services said.
Filefax, Inc., located in Northbrook, Ill., closed in 2016, while it was under investigation by HHS' Office of Civil Rights for HIPAA infractions that occurred in early 2015.
HHS received an anonymous complaint on Feb. 10, 2015 claiming that Filefax had taken medical records to a shredding facility earlier that month but failed to properly dispose of the documents, which contained protected health information from about 2,150 patients.
A subsequent investigation by OCR found that in January and February 2015 Filefax had left those patient medical records in an unlocked truck in the company parking lot.
"The careless handling of PHI is never acceptable," said OCR Director Roger Severino. "Covered entities and business associates need to be aware that OCR is committed to enforcing HIPAA regardless of whether a covered entity is opening its doors or closing them. HIPAA still applies."
In 2016, in unrelated litigation, a court appointed a receiver to liquidate Filefax's assets for distribution to creditors. In addition to a $100,000 settlement, the receiver has agreed to store and dispose of remaining medical records found at Filefax's shuttered facility in compliance with HIPAA.
When the deals are finalized, CityMD will have 100 urgent care centers in the New York Metropolitan area. CityMD has grown by more than 40% in the past year.
CityMD's aggressive expansion continues with the acquisition of STAT Health, an urgent care provider with 12 clinics on Long Island, and FirstMed Immediate Medical Care, an urgent care center in Queens, the company announced Tuesday.
Financial terms were not disclosed for either deal, both of which are expected to be finalized by the end of March.
When the two acquisitions are in the books, Manhattan-based CityMD will have 100 urgent care centers in the New York Metropolitan area. STAT had plans to open two more urgent care centers this year in Nassau and Suffolk Counties, and that plan will continue under the CityMD brand.
"I am thrilled to be reaching this milestone of 100 CityMD locations, and excited to welcome STAT Health and First Med to the CityMD team," CityMD CEO Richard Park, MD, said. "Our seamless integration will enable us to serve more patients in Eastern Long Island and Queens, and bring us closer to achieving our vision of building healthier, kinder communities."
Last year Warburg Pincus bought a majority stake in CityMD, which was founded in 2010. CityMD has grown 43% since then, and now includes more than 400 providers in its network.
STAT Health was founded in 2005 by Paolo Coppola, MD, who grew the company to include eight clinics on Long Island. Plans were underway to double the size of STAT Health after partnering in 2016 with the investment firm Spanos Barber Jesse & Co.
The two companies have also entered a seven-year agreement that makes Press Ganey's curriculum available exclusively on HealthStream’s workforce training platform.
Nashville-based HealthStream is selling its Patient Experience platform to Press Ganey Associates for $65.5 million in cash.
The two companies also announced that they have begun a seven-year deal that makes Press Ganey's curriculum, courses and certificate programs available exclusively on HealthStream's workforce training platform.
"Press Ganey is passionate about advancing patient-centered care supported by a high performing workplace," Press Ganey CEO Patrick T. Ryan said in a media release.
"We have great respect for the partnerships that HealthStream has developed with its patient experience and engagement clients and look forward to adding these organizations to Press Ganey's transformative platform," Ryan said. "We are committed to ensuring a seamless transition and to partnering in their mission to deliver safe, high-quality, patient-centered care."
HealthStream started PX in 2005 when it bought Data Management & Research Co.
In a separate announcement, the two companies said that all of Press Ganey's newly acquired Patient Experience Improvement and Engagement libraries will be available to HealthStream customers. Both companies will sell Press Ganey content through HealthStream-powered applications.
"Although we are divesting our PX business to Press Ganey Associates, we are entering into a new strategic collaboration with them," HealthStream CEO Robert A. Frist, Jr. said.
"HealthStream is pleased to add Press Ganey to its growing network of outstanding healthcare content providers—the industry's broadest selection of thought-leading content from among leading healthcare associations, medical publishers, and nursing associations," Frist said.
The budget deal passed by Congress delays for two years $2 billion in cuts to disproportionate share payments. Safety net providers say that the additional time can be used to fashion a long-term solution for uncompensated care costs.
The two-year delay in disproportionate share payments is a credit positive for the nation's safety net hospitals, Moody's Investors Service said.
The $2 billion in cuts representing 17% of the federal Medicaid DSH budget were mandated in the Affordable Care Act, and were supposed to take effect on Oct. 1, 2017, the start of federal fiscal year 2018. But Congress on Friday passed a budget that extends the life of the payments for another two years.
"This development restoring DSH payments is credit positive for safety net hospitals that treat large numbers of indigent patients and often rely on various supplemental payments or direct government subsidies," Moody's said. "It is also credit positive for states and local governments that own safety-net hospitals or that provide significant funding to local safety nets, including local governments in New York State, California and Texas."
About 2,700 hospitals across the nation get DSH money, although payments vary significantly. Safety-net hospitals that have high volumes of Medicaid and uninsured patients generally receive the bulk of DSH payments.
Medicaid and the Children’s Health Insurance Program Payment and Access Commission report that 37% of the hospitals most reliant on DSH funding are publicly owned and receive 80% of all DSH payments, improving margins by an average 6.4 percentage points.
Bruce Siegel, MD, president and CEO of America’s Essential Hospitals, said Congress "made the right choice" in delaying the DSH cuts. The additional time, he said, "gives hospitals and policymakers time to find a long-term solution to uncompensated care costs, which threaten access to care in communities nationwide."
"Essential hospitals provide high-quality care for all people, regardless of their health needs and financial and social status. To continue meeting this mission, these hospitals need stable, sustainable federal support," Siegel said.
The Jackson, Michigan–based health system agrees to stop coordinated anti-competitive business activities with competitors, but insists that it did nothing wrong.
Henry Ford Allegiance Health has settled its three-year antitrust fight with state and federal prosecutors, just weeks before the case was set for trial in federal court.
The Department of Justice and the Michigan Attorney General’s office filed suit in 2015, alleging that Henry Ford Allegiance Health and three other health systems in south central Michigan carved up the territory and insulated themselves from competition by agreeing to withhold outreach and marketing in each other's respective counties.
The three other health systems, Hillsdale Community Health Center; Community Health Center of Branch County in Coldwater; and ProMedica Health System in Toledo, OH, settled their suits two years ago.
"As a result of Allegiance's per se illegal agreement to restrict marketing of competing services in Hillsdale County, Michigan consumers were deprived of valuable services and healthcare information," Assistant Attorney General Makan Delrahim in DOJ's Antitrust Division said in a media release. "By prohibiting further anticompetitive conduct and educating Allegiance executives on antitrust law, this settlement will ensure that consumers receive the fruits of robust competition."
The proposed settlement was filed Friday in U.S. District Court for the Eastern District of Michigan, where the case was scheduled to go to trial on March 6.
Allegiance said in prepared remarks that it felt compelled to settle even though it did nothing wrong.
"We reluctantly chose to settle this litigation because continuing to defend ourselves against the United States and State of Michigan became too costly," the health system said. "This decision, regrettable but necessary, requires us to discontinue our defense of this case before the Court could rule on any of the highly contested issues raised in the litigation."
DOJ’s settlement with Allegiance expands on the earlier settlements with the other three health systems, which means that Allegiance cannot communicate, coordinate or limit marketing or business development with competitors. The agreement ends the health system’s carve out in Hillsdale County. Allegiance must also file annual compliance reports and submit to compliance inspections, and reimburse state and federal prosecutors for the court costs.
DOJ said the deal includes several new provisions that are now included in all new consent decrees that add greater specificity and accountability.
"The proposed settlement will make it easier and more efficient for the department to enforce the decree by allowing the department to prove alleged violations by a preponderance of the evidence," Delrahim said. "These provisions will encourage a stronger commitment to compliance and will ease the strain on the department in investigating and enforcing possible violations."
Patricia Wagner, an antitrust attorney with Epstein Becker Green and a disinterested observer, said DOJ is applying more rigorous benchmarks for its consent decrees.
"When you do your annual report you have to document that everybody got their four hours of training and you have to provide the materials that were used in those training sessions. If DOJ asks, you'd have to provide a lot of who had what conversations, and when," Wagner said. "Instead of just having a general 'you will comply with this consent order and verify annually that you are doing so,' it is giving organizations the steps that DOJ thinks they need to take in order to comply with the consent judgements."
"If I am a CEO of a hospital maybe I am thinking about how to get ahead of this situation. Should I have someone who is responsible for antitrust compliance?" she said. "All hospitals have large compliance programs that are usually focused, as they should be, on fraud and abuse and licensure issues. It seems like a natural evolution to say 'maybe we should be thinking about including antitrust in that larger compliance program.'"
Henry Ford Allegiance Health operates the only hospital in Jackson County, MI. The system also operates primary care, physical rehabilitation, and diagnostic facilities in several counties in south central Michigan. Allegiance joined Henry Ford Health System in 2016.
Allegiance’s statement in full reads as follows:
Allegiance Health and the Department of Justice have settled an antitrust case brought by the DOJ against Allegiance Health in 2015. The original complaint alleged that Allegiance Health entered into an agreement with Hillsdale Community Health Center to limit marketing in Hillsdale County.
We reluctantly chose to settle this litigation because continuing to defend ourselves against the United States and State of Michigan became too costly. This decision, regrettable but necessary, requires us to discontinue our defense of this case before the Court could rule on any of the highly contested issues raised in the litigation.
We still deny unlawful conduct of any kind, and the settlement does not include any admission of liability. Despite almost three years of litigation, there was no finding of wrong doing by the Court, and, as recently as December, the Court contemplated dismissing the action in its entirety. In addition, the Court has never ruled that the citizens of Hillsdale County were harmed by our marketing strategy.
We reaffirm our belief that we promoted competition in south central Michigan and benefitted the citizens of Hillsdale County in undeniable ways. The terms of the settlement allow us to continue our marketing strategies in order to best serve the people of south central Michigan including Hillsdale County.
NIH study finds effective surveillance efforts for drug-resistant organisms minimize patient infections, even close to a reservoir of resistant bacteria.
Hospitals do a good job killing antibiotic-resistant organisms in high-touch areas such as counter tops, doorknobs, computer keyboards, and sinks, a new National Institutes of Health study says.
However, drainage pipes under hospital intensive care units, and in outside sewers that collect hospital wastewater are teeming with those organisms, including bacterial plasmids that confer resistance to carbapenems, the "last-resort" antibiotics given to hospital patients who develop infections from pathogens that are multidrug-resistant, the researchers report in mBio.
"Strikingly, despite a very low prevalence of patient infections with blaKPC-positive organisms, all samples from the intensive care unit pipe wastewater and external manholes contained carbapenemase-producing organisms, suggesting a vast, resilient reservoir," the study said.
That comparison suggests that surveillance efforts to watch for resistant organisms minimize patient infections, even so close to a reservoir of resistant bacteria, says NIH microbiologist Karen Frank, who co-led the study.
"If you're tracking resistant bacteria, you might be able to prevent more infections in patients," she says.
The study also raises an important question.
"How much should we care that there are a bunch of plasmids down in the wastewater system if they're not infecting our patients?" Frank says.
The new findings add to growing evidence suggesting that the conduits of hospital wastewater serve as a vast, resilient reservoir for plasmids that can confer the genes responsible for antibiotic resistance.
Frank says these populations flourish in wastewater because of the common use of strong antibiotics in hospitals, which leads to an uptick in antibiotic-resistant microbes in the sewers.
"The bacteria fight with each other and plasmids can carry genes that help them survive," she says.
As part of a complex bacterial community, they can transfer the plasmids carrying resistance genes to each other, which means that the bacteria can gain resistance without exposure to antibiotics.
NIH researchers compared their data to five years' worth of patient data and samples collected from sinks and other high-touch areas, like countertops, door knobs, and computers. Remarkably, the high prevalence of carbapenem-resistant plasmids in the pipes and sewers wasn't seen in parts of the hospital to which patients had access. Of 217 samples analyzed from high-touch surfaces, only three (1.4%) tested positive for carbapenem-resistant organisms. Similarly, of 340 samples collected from drains, only 11 (3.2%) were positive.
Frank says understanding the plasmid exchange and when the plasmids get into the pathogens that infect our patients could help hospitals improve their monitoring of resistance-conferring genes.
"In the big picture, the concern is the spread of these resistant organisms worldwide and some regions of the world are not tracking the spread of the hospital isolates," she says.